Nosokinetics
December 2005 Issue
(c)Authors for content; Peter Millard, Roy Johnston for e-version
(comments to rjtechne at iol dot ie)
What's in a word: Nosokinetics?
Although millions of people know that MRSA infections are acquired in hospitals, few would recognise this if they were told MRSA is a nosocomial infection. Two years after we launched Nosokinetics News we now have 115 hits on the web. Contrast that with the 2,160,00 hits for MRSA and you can see that we have a long way to go.Should we have started from here? At the end of our second year, I think of the car-driver lost in a Irish village who asked an old man sitting on a seat "How do I get to Dublin from here?" Only to be told, "I wouldn’t start from here if I were you."
Hospital acquired infections, drug errors, bed shortages, bed borrowing, bed blocking, outliers, trolley waits, ambulance by passes, cancelled operations, delayed discharges and constant managerial changes plague modern hospitals. The rationale for what we do is clear: "It's an interesting problem, which for everyone's benefit needs to be solved."
Moreover, in the United Kingdom, since the 1980s, bi-annually, government Ministers have been changing the way the NHS is organised, thus giving the illusion of progress while causing the maximum confusion and dismay. Will we solve that? It's a tall order, yet, "If the flapping of a butterfly's wings in the Amazonian jungle can cause a hurricane in the Pacific Ocean" who knows what can be achieved.
As the New Year approaches may I take this opportunity to thank you for your support and to wish you good fortune and good health in 2006 and beyond.
Footnote: "A Sting in the Tale" A reader writes: It's an uphill struggle. At a Strategic Health Authority meeting on capacity planning, the organiser stated that (Episodes) * (80th percentile of LOS) was the ONLY way to calculate bed requirements. When I argued that whilst the 80th percentile was better than the average, there are considerably better ways of estimating bed requirements. I was told to shut up because "The NHS is not ready for your way of thinking"
Nosokinetics on the web - last but not least:
MRSA (2,160,000 Google hits)
Nosocomial (940,000)
1. Of or pertaining to a hospital; as nosocomial atmosphere
2. Acquired in a hospital; as a nosocomial infection
Nosology (78,800): A systematic arrangement, or classification, of diseases
Nosological (36,100): Of or pertaining to nosology
Nosography (9,600): A description or classification of a disease
Nosopoetic (2,330): Producing diseases
Nosophobia (716): A morbid dread of disease
Nosokinetics (115): The science/subject of measuring and modelling flow in health and social care systems
Simulating Accident and Emergency Services with a generic process model; Anthony Codrington-Virtue
Patients enter and leave hospitals 24 hours a day throughout the year. As well as purpose, structure and function model makers need to consider time, day and method of arrival, degrees of difficulty, age, alternative placement and staff availability. Here research developing a generic process of accident and emergency services is described. Data analysis is important. Look and see how the four hour (political) waiting list targets distorts the pattern of length of stay.
Outpatient Models for a Diagnosis and Treatment Centre: John Bowers and Gillian Mould
Staff from the University of Stirling have been working with Hospital Trusts to produce tools to support the modernisation of health services. Past studies have explored day surgery and inpatient care. A recent project has focussed on outpatients, developing models to assist in the design of a Diagnosis and Treatment Centre (DTC). A planning tool has been constructed which allows managers to select the specialties for inclusion in the DTC and explore the consequences.
Leaving emergency departments without being seen.
Modelling emergency department capacity, Polevoi S. et al. (2005); Academic Emergency Medicine 12, 232-236: report that emergency department capacity of 100% may not be a sensitive measure for overcrowding. Physician factors, especially emergency medicine training, also appear to be important. Greater than 100% occupancy is associated with patients who leave and this is most significant at 140% capacity. Physician factors, especially emergency medicine training also appear to be important when using Leave Without Being Seen as a performance indicator.
Statistical methods for length of stay
E Kulinskaya, D Kornbrot, H Gao: Length of stay as a performance indicator: robust statistical methodology. IMA Journal of Management Mathematics 2005, 16:369-381.Robust statistical methods are required because outliers bedevil the statistical analysis: they influence the mean (average stay) so their presence in the calculation has unfortunate consequences for 95% of patients who are not outliers. To determine the most appropriate statistical analysis for LOS data, using health care statistics from the UK NHS for 1997/98, standard general linear models were compared with an advanced robust method called truncated maximum likelihood.
New findings were that admission method, discharge destination, provider (hospital) type, specialty and NHS region all influence length of stay, e.g., LOS is 25% longer for patient transferred from other hospitals rather than those admitted as an emergency. Also, death occurs early and transfer occurs late. Since the new NHS case mix funding ignores transfers and destination at discharge, while encouraging shorter length of stay, trusts with higher mortality may be doing the best under the new system. Which is certainly not desirable from the patient’s point of view. Editor's comment. The results are clinically not incorrect, the paper charts a new way forward and needs wider dissemination.
Nosology on the web
PP Levy: The case view, a generic method of visualization of the case mix. Int J Med Inf 2004, 73:713-718.Hundreds of DRGs are described in tables, how do you sort them? Pierre Levy's method has developed a fascinating nosological way. Sort the DRGs by their cost into three groups – low, medium and high. Allocate a pixel to each DRG according to their cost group. Then sort the pixels by their colour group and visually display the results using ten columns each corresponding to a major category of diseases or to clusters of major categories. The display shows immediatiely that most of the DRGs are medium costs, that the costly DRGs are mainly surgical, and that the "ambulatory" zone contains a certain number of medium cost DRGs and that there exists low cost DRGs in the non ambulatory zone. Editors comment: Have a look at this one it's fascinating.
MASH NET Launch report
MASHnet - The Network in Healthcare Modelling and Simulation was established on January 4th 2005 after receiving grant funding from the Engineering and Physical Science Research Council for £60 thousand pounds for three years.Mashnet Aims To improve the application of modelling and simulation techniques within healthcare decision.
Slides of presentations and notes of group discussions at the MASH net Launch event 'MODELLING HEALTH CARE - making it work' held on Tuesday 20th Sept 2005 at Warwick University are on the web. Follow the link for the speakers’ contributions in pdf.
Modelling and Simulation in Health - Potential, Achievement and Challenge.
Dr Geoff Royston, Head of Operational Research, Department of Health, gives background information on recent major developments in UK health care and a short overview on modelling, and simulation in the UK health sector, including some from the work of OR analysts in the DH. Finally, he highlights some key issues for the UK health sector in the early 21st century and the challenges and opportunities these present for members of MASHnet.
OR, Academics and the Health Service
Professor Ruth Davies, Head of the Operational Research and Information Systems Group at Warwick Business School considers the relationship between OR and the Health Service using a hospital and a disease based case study. Demonstrating that academic research needs to take a broad view, both developing and exploiting new techniques and also taking account of the objectives of a range of stakeholders. Whilst academics are also concerned with implementation and change, they and the "users" will benefit from closer links with practitioners and software developers. We anticipate that MASHnet will facilitate this.
Developing Models of Health.
Dr Mark Elder, CEO of SIMUL8 Corporation, founded the company in 1994 because a radiology manager could not find simulation software that could answer his simple question: "Should I build an additional radiology room, or hire an additional nurse?" Using recent examples of healthcare simulation models Mark highlight some do's and don'ts in simulation modeling, before considering the numerical and non-numerical benefits of spending time on modelling.
Designing win-win-win solutions for improved healthcare performance - it is possible!
Dr Simon Dodds, Consultant Vascular Surgeon at Good Hope Hospital, Birmingham combines his experience in medicine, research and computer science to improve vascular surgery services at Good Hope. Simon argues that the current challenges in delivering high quality, cost effective, healthcare is not lack of medical knowledge but ineffective delivery of existing knowledge. Applied OR has great potential to dramatically improve existing services. Using Discrete Event Simulation a possible increase of 40% in maximum clinic capacity using existing resources was predicited. Implementing the best model in practice - resulted in a win-win-win outcome for patients, staff and the hospital.Caution is needed, however, for the principles and methods of OR/OM require specific knowledge, skills and experience to apply safely. Active diffusion of innovation requires - support for further innovation, appropriate software tools, end-user training, and a programme of training successive waves of early adopters. The goal is the tipping point where the momentum generated is sufficient to complete the paradigm shift to a culture of evidence-based healthcare management. Further details about the aims of MASHnet can be found on the website or by emailing mashnet@PenTAG.nhs.uk.
IT's the FESTIVE SEASON - XYZ.
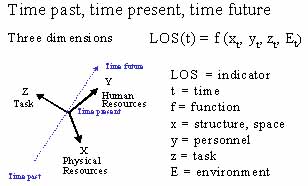
This is the nosokinetics challenge. Thierry Chaussalet developed it for our paper at the Hawaii conference. Everything we do stands on a moment of time. In that moment we are influenced by what happened in the past, where we are now, and what will happen in the future. Solve resource allocation with a random allocation clinical trial and you really are a magician. Far from being the gold standard, such trials are fool's gold.
R Rosenthal, L Jacobson: Pygmalion in the classroom: Rinehart and Winston Inc.; 1968.
We are indebted to IMS MAXIMS plc's sponsorship for enabling the website version to be developed. IMS is a significant supplier to NHS and has an ongoing interest in enhancing the scope of IT support in the NHS, especially in the areas of clinical knowledge and decision support. Developers of systems looking for market opportunities are invited to contact IMS at their UK office, or by e-mail to Paul Cooper (pcooper at imsmaxims dot com). Accessing their web-site http://www.imsmaxims.com> will give a feel for the scope of their work.
Some navigational notes:
A highlighted number may bring up a footnote or a reference. A highlighted word hotlinks to another document (chapter, appendix, table of contents, whatever). In general, if you click on the 'Back' button it will bring to to the point of departure in the document from which you came.Copyright (c)Roy Johnston, Ray Millard, 2005, for e-version; content is author's copyright,