Nosokinetics
Post HSCM2006 thoughts on scoping the Nosokinetics approach
John O'Brien, Director, Epidemiology Services, Queensland Health, Australia
(comments to rjtechne@iol.ie)HSCM2006 in Adelaide brought together an interesting group of 'bedfellows', who are destined to become known in the future as 'nosokineticists' (OED compilers - please note - first usage 2006!). Attenders came principally from the health and ageing sectors, but represented a wide range of clinical and managerial interests - from acute care, chronic/aged care, accident and emergency departments, elective surgery, outpatient management, primary health care, mental health, rehabilitation, and palliative care. The conference showcased a range of interesting tools for modelling, simulation, scenario planning and scheduling and evidence of their application in clinical management, service and workforce planning, and resource allocation. There are probably no surprises that nosokinetics - the science/subject of measuring and modelling flows in health and social care systems - had its origins at the junction of geriatrics and aged care, as these are among the areas of greatest competition for 'beds', but the broad definition that has evolved may allow a more inclusive scoping of the science. Occupied Bed Days and Length of Stay are critical to the clinician/manager who is trying to balance demand and supply in a ward, but nosokinetics may permit us to work with a much wider range of metrics.
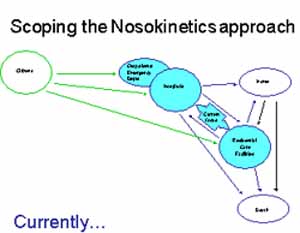
Fig 1: Current scoping.
Contemporary practices in chronic disease management mean more services are being provided in primary health care settings, where similar pressures of need and demand outstripping supply and capacity also apply from time to time. Clinical pathways and management plans, along with examples of sophisticated and systematic use of data linkage, could lead us to a better understanding of the health trajectories of individuals and their likely need for services.
There is already a substantial body of work - represented at the Adelaide conference - on potentially preventable admissions and emerging work on the cost-effectiveness of strategies to achieve reductions in these areas.
Patient/client flows inside health and residential care facilities are definitely within the scope of nosokinetics, but what about encounters with primary and community-based health and health-related services.
Would an expanded scope - including flows through primary health care services and linked to hospital episodes - be valuable in understanding the burden of disease and the dynamics of health system responses?
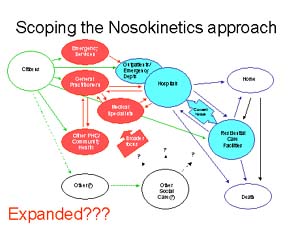
Fig 2: Revised scoping?
Nosokinetics is potentially a discrete discipline, rather than a 'grand theory' for the health of populations. But, with the judicious use of data linkage and smart cards, could it help us build a comprehensive framework for understanding flows within health and social care systems - beyond the hospital gates?
Ed's note - discussion in these pages is welcomed!
Some navigational notes:
A highlighted number may bring up a footnote or a reference. A highlighted word hotlinks to another document (chapter, appendix, table of contents, whatever). In general, if you click on the 'Back' button it will bring to to the point of departure in the document from which you came.Copyright (c)Roy Johnston, Ray Millard, 2005, for e-version; content is author's copyright,