Nosokinetics
Electronic Issue October 2007
(c)Authors for content; Peter Millard, Roy Johnston for e-version
(comments to rjtechne at iol dot ie)Editor's introduction
In this issue: Two Mark's, both Australian - Mark Fackrell, Melbourne, continues his phase-type tutorials; Mark Mackay, Adelaide, considers "How can we open the door?". From Thierry Chaussalet's group, FLoSC, a tool to forecast length of stay and costs in social care is described. Shola Adeymi, PhD student, reveals some mathematical mysteries in modelling pathways. I muse about medieval fish traps, bed-blocking and the tide coming in. Ludwig Kuntz's research into the process of care in German hospitals. And we give details of abstract submission and registration for HSCM2008 being organised Sally McClean at the University of Ulster.
Congratulations to Mark Mackay His University of Adelaide, PhD thesis on "Compartmental Modelling of Acute Care Hospital Bed Occupancy for Strategic Decision Making" has passed the exam, with minor alterations. Once those are done we can then, happily address him as Dr. Mark Mackay, and put the abstract into the newsletter. Mark's original contribution is to demonstrate, using data from Australia and New Zealand, the applications of compartmental flow modelling to forecasting in long term and short term outcomes of change.
Phase-type Distributions in Healthcare Modelling 2
Mark Fackrell, Dept. of Mathematics and Statistics, University of Melbourne, AustraliaThe second of Marks' three articles on phase-type (PH) distributions, attached to this newsletter in a pdf file, describes Coxian distributions. These special types of PH distributions are particularly useful in health care modelling.
Figure 1 shows the state transition diagram for an order p Coxian distribution. Notice that the representation (1)-(2) depends on only 2p-1 parameters, whereas General PH representations require p2 + p - 1 parameters. Thus general PH distributions are over parameterized, whereas Coxian distributions are not.

Figure 1: state transition diagram for an order p Coxian distribution.
The shapes in Figure 2, from a three order 4 Coxian distribution with the same generator, but different vectors, exhibit much more flexibility than an exponential function, which should come as no surprise as they rely on 7 free parameters instead as just one! Indeed Coxian distributions are more versatile than both hyperexponetial distributions and generalized Erlang distributions, which also depend on 2p-1 parameters.
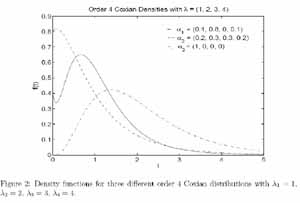
Figure 2: three order 4 Coxian distributions with the same generator.
Mark illustrates the use of Coxian distributions with the state transition model used by researchers from the HSCMG at the University of Westminster. By coincidence, serendipity, no editor's tricks were involved.
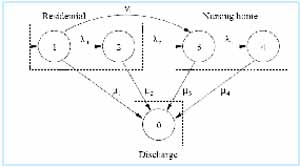
Figure 3: state transition model used by researchers from the HSCMG.
Also see FLoSC elsewhere in this Newsletter showing the practical potential of this modelling tool.
The full text of Mark's paper is in the IMS archive (see below) and in the Tutorial section of the Nosokinetics website at http://www.nosokinetics.org.uk/.
Looking in from the outside - time to get through the door
Mark Mackay, Principal Project Officer, Department of Health, South Australia.Editor's comment: Medicine used to be an Art based Science, now it's a Science based Art. Mathematical modelling is not a forest fire. Indeed its opaque, but as Haifeng Xie said one day, "Maths is boring, but there are exciting things you can do with it". Given, for every equation one has in a paper", Sally McClean says "You loose 50% of the readers". There is a brave new world, shorn of constant change, but "How do you get the message across?" Also see MASH News in the 2006 August (3.4) Nosokinetics News.
Academic research to practical use: A step forward by the HSCMG
Research by the Health and Social Care Modelling Group (HSCMG) at the University of Westminster, in collaboration with the London Borough of Merton, has led to the development of a practical decision support tool FLoSC, which is a toolkit helping Local Authorities to analyse the patterns of length of stay of their publicly funded clients in institutional long-term care.FLoSC forecasts the cost of existing, known commitments i.e. how much money will be needed this year and in future years for the group of publicly funded residents currently in residential and nursing home care. So, using their data, local authorities can estimate the money available for new admissions and determine how much of next year's budget is available for home and institutional care. The toolkit can also be used to compare forecasts under different cost scenarios, which may reflect possible future changes in pricing or costing policy. These functionalities are of crucial importance to the planning of a successful budget for long-term care at local authority level.
The development of FLoSC was funded by the Care Services Efficiency Delivery http://www.csed.csip.org.uk/ program of the Department of Health, UK.
For upcoming information and updates about FLoSC, please visit visit http://www.healthcareinformatics.org.uk/ or email Thierry Chaussalet (chausst at wmin dot ac dot uk).
Patient flow: A mixed-effects modelling approach
Shola Adeyemi, PhD student, HSCMG, University of Westminster, UKIntroduction: In the studies of patient flow and LOS modelling, an individual patient's experience during the delivery of care is often overlooked. In order to have an insight into what an individual patient might experience during the course of care, we propose a modelling framework for patient pathways through the healthcare system based on mixed effect models.
Modelling approach: Health care delivery can be seen as a multi-state system; a patient's experience in the system is captured by the different states (locations or health states) visited by the patient. This is also known as patient pathway, which essentially is a collection of clustered or repeated observations of a patient. Mixed effect models, which incorporate fixed effects (e.g. the systematic component capturing the population correlation structure) and random effects (e.g. the random component capturing patient specific effects) are naturally suited in such a modelling situation.
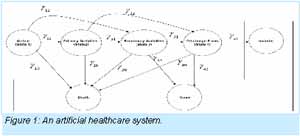
Figure 1: artificial healthcare system.
We illustrate this modelling concept using an artificial healthcare system depicted in Figure 1. We assume that patients entering the system will undergo some interventions and then progress from doing primary, secondary and discharge planning activities before discharge, which includes discharge by death, discharge to patients' home or transfer to another healthcare institution. In a (non-absorbing) state, we model the probability of going through any path (e.g. an outgoing arrow) using a multinomial formulation. Furthermore, we introduce the concept of health status of a patient, which is modelled as a random effect. The idea is that health status of a patient is the underlying driving force of movements in the system. Health status can be further modelled by a set of covariates if such data is available.
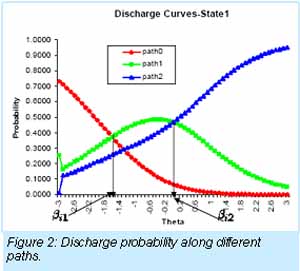
Figure 2: changes in the health status.
For illustration, Figure 2 show the effects of changes in the health status of a patient on the probability of discharge in state 1. Since there are three paths leaving the state, there are two threshold values (e.g. ??? and ???) (??) for the health status value of a patient, above which the likely path will change. In this case, path 0 and path 1 intersect at ??? = -1.5, and path 1 and path 2 intersect at ??? = 0.1. These thresholds show that the most likely path is path 0 when a patient's health status measure is below ???; and path 1 is the most likely between ??? and ???; while path 2 is the most likely above ???. Note that if ????< ???, it suggests that path 1 will not be most likely at any point. This might be interpreted as indicating a problem with path 1. However, this is not always the case.
Conclusion: We have demonstrated that mixed effect models can play an important role in modelling patient pathway. Further work is currently underway to improve this modelling framework. For more detail of the model, please see:
Adeyemi, S., Chaussalet, T., Xie, H. and Millard, P. (2007) Patients flow: a mixed-effects modelling approach to predicting discharge probabilities. In: Proceedings of the 20th IEEE International Symposium on Computer-Based Medical Systems, pp. 725-730, IEEE CBMS 2007, Maribor, Slovenia, 20-22 June 2007.
Global warning: high tide is on its way; old people are coming and they won't go away
Peter MillardCampervanning on the Isle de Reé, on the Atlantic coast of France. Banned from internet cafes, no emails what bliss. Reading Preserved Smith's (1934) History of Modern Culture, 1678-1776, as one does, thinking about the enlightenment that followed Newton's laws. Looking at nature stacking sea shells on plants and exploring medieval fish traps, my thoughts turned to ‘bed blocking' and the computational and conceptual errors that underpin the world wide crisis in hospital care.

Figure 1: caption?
The Isle de Ré, is only 30 kilometres long and 5 kilometres wide with no hills. It's a cyclists paradise. It has no hills and separate cycle tracks. Moreover, there are bicycle hire shops in all the villages and, when tired, buses to bring you and the bike back to the base. Moreover, it has a fascinating history. Both as a military base protecting La Rochelle, and as a source of salt and fish.
"What's that to do with Nosokinetics?" you may well ask. Well in the middle ages the island had 141 fish traps, now only six remain. Built and repaired by hand, damaged frequently by the storms, both little and big fish are caught as they come in on the tide. Vertical Iron bars at the ‘holes in the walls' ensure that big fish stay in and little fish are netted as they go out with the tide. So, that's a two compartment model if ever I saw one.
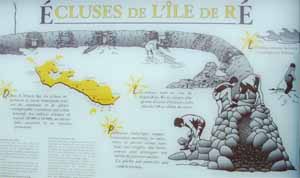
Figure 2: caption?.
Later we visited the museum of the sea and saw for the first time the mathematics of the tides. Analogies abound. Could the mathematics of the rising and falling tides be adapted to help solve the problem of seasonality in hospital care. High tides midday, low tides at night.
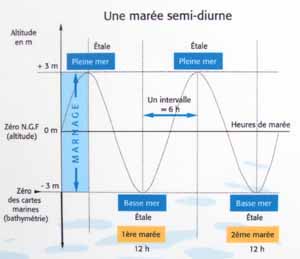
Figure 3: caption?.
Everyone knows that rivers are more likely to break their banks and overflow at midnight. So defences are planned accordingly. Why then is hospital bed occupancy still measured in nights?
Also days of the week and seasons of the year influence the need for acute hospital care? The modern emphasis is on fast track treatment and plans are being made accordingly. But, how can you plan for that if you don't know the hour at which in patients arrive and leave.
So errors abound. Like the tidal seas, hospital beds are never completely empty and different numbers and types of big and little fish come in with the tide.
Until we recognise the need to measure the process of patient care in minutes, hours, days, weeks, months and years, the medieval fist traps tell us we will never solve the problem of care. Also, like the fish traps, comprehensive hospital and community services take years to build and days to smash down.
Modernising Acute Hospital Care: Reviews
Editor's comment. If you are interested in the management theories that underpin the modernisation of acute hospitals, three recent papers from Ludwig Kuntz' group are well worth reading. They opened my eyes.
Incorporating efficiency in hospital-capacity planning in Germany:
Kuntz, L., S. Scholtes, et al. (2007). European Journal of Health Economics 8(3): 213-2
Bed occupancy, as a measure of hospital efficiency, neglects important drivers of economic efficiency, such as treatment costs and case mix. An alternative metric is developed and used in the hospital-capacity planning cycle in a German federal state. 92 hospitals were involved. Standard hospital data, including annual costs, number of cases, disaggregated by medical departments, ICD codes, length-of-stay, certified beds, and occupancy rates were used. 18 hospitals were deemed to be inefficient and targets for over-proportional capacity cuts and 15 were identified as efficient hospitals. The developed model and analysis has affected the federal state's most recent medium term planning cycle.
Process-Based Organization Design and Hospital Performance:
Vera, A. and L. Kuntz (2007). Health Care Management Review 32(1): 55-65.
Lean thinking, continual quality assurance, six sigma are all forms of process based change. The economic aim being to drive down costs, while improving quality of product, i.e. satisfied customers buying the product. The research hypothesis was "Hospitals that exhibit a high degree of process orientation in their organization design are more efficient than hospitals with a low degree of process orientation". Using data development analysis, factor analysis and regression analysis and data gathered by questionnaire from 43 chief executives the researchers found had a high degree of process-based-reorganization has a moderate but significant positive effect on efficiency. With the caveat, that implementation rules, physician involvement and an adequate organizational culture are essential components of success.
Modular organization and hospital performance.
Kuntz, L. and A. Vera (2007). Health Services Management Research 20: 48-58.
Modularization is a modern form of organization, which vertically disaggregates a firm and uses market mechanisms within hierarchies. This paper examines whether the use of modular structures has a positive effect on hospital performance. Using multiple regression analysis, the main result is that modularization does not have a positive effect on hospital performance. However positive efficiency effects of two central ideas of modularization, namely process orientation and internal market mechanisms were found..
BUILDING ON EXPERIENCE
on WEDNESDAY, NOV 21st 2007
at UNIVERSITY OF WESTMINSTER, LONDON
The cost for the day will be Ł40 for bookings received before Nov 1st (Ł50 after that date). This will include refreshments during the day and full buffet lunch. Places are limited to 80 participants and early booking is advised.
(Email enquiries can be directed to: joanne.perry@pms.ac.uk)
(HSCM 2008)
Portrush, Northern Ireland 18 - 20 March, 2008
http://info200.infc.ulst.ac.uk/events/hscm2008/themes.html (for Paper - Submission)
The conference fee includes two nights accommodation, and full board at the Comfort Hotel at the Ramada hotel in Portrush http://www.comforthotelportrush.com , a small seaside town on the North Coast of Ireland, with beautiful beaches, convivial restaurants and friendly pubs. It is close to the Bushmills Distillery and Giant's Causeway and part of the Causeway Coast Area of Outstanding Natural Beauty.
Abstract Submission: 30th October 2007
Abstracts of one A4 page are invited for oral or poster presentation. Format: Font Times New Roman 12 point, 1.5 spacing, single column, margins: left 3cm; right 2.5cm; top & bottom 3cm; file type MS Word (preferred).
Please submit your abstract by email to Sally McClean at si.mcclean@ulster.ac.uk
Acceptance Notice: 23rd November 2007
Registration Early-Bird Deadline: 30th November 2007
Seeing one self as others' see us
Adele kindly bought this model of an old doctor in America and gave it to me. I leave it to you to guess what the old doctor is going to do next.However, the words on the plinth "Old doctor's never die, they only loose their patience" reminded me of a ward round in 1974. Surrounded as we were then, ‘God going round with his angels' - junior doctors, medical students, nurses, therapists, I said to a lady of 104:
."You can go home on Monday and I will arrange, home help, district nurse and meals of wheels for you". She replied "Don't be such a stupid little boy. Monday is not convenient for me and I am perfectly capable of making my own social arrangements." Then with a sweet smile, she ended ‘Thank you for getting me better.'
We are indebted to IMS MAXIMS plc's sponsorship for enabling the website version to be developed. IMS is a significant supplier to NHS and has an ongoing interest in enhancing the scope of IT support in the NHS, especially in the areas of clinical knowledge and decision support. Developers of systems looking for market opportunities are invited to contact IMS at their UK office, or by e-mail to Paul Cooper (pcooper at imsmaxims dot com). Accessing their web-site http://www.imsmaxims.com will give a feel for the scope of their work.
Some navigational notes:
A highlighted number may bring up a footnote or a reference. A highlighted word hotlinks to another document (chapter, appendix, table of contents, whatever). In general, if you click on the 'Back' button it will bring to to the point of departure in the document from which you came.Copyright (c)Roy Johnston, Ray Millard, 2005, for e-version; content is author's copyright,